The Medfield Fire Department runs an Emergency Medical Service (EMS), staffed by EMT’s (Emergency Medical Technicians), who are also firefighters. We have historically utilized Advanced Life Support (paramedic) intercepts – i.e. the MFD EMT’s will begin the patient transport and transfer the patient to the ALS ambulance when the ALS ambulance intercepts the MFD ambulance on the way to the hospital. However, within the past two months, two ALS services have cancelled their ALS intercept services with Medfield, because the intercepts were not making enough money, and as a result we currently have no ALS intercept service,. And we are told, with the economies making it unlikely that there will be any new ALS offers.
Our EMT’s now transport patients all the way to the hospital. So what is the difference? MFD ambulance EMT’s offer fewer services to someone than a paramedic could supply. As I understand the differences, it is mainly in the ability of paramedics to administer medications, provide shots, and insert IV’s.
Like the author of the email below, I personally met a young Medfield man, at a BSA event, who I was told is alive today, after his heart stopped, only because he was revived by paramedics.
The town will need to make the decision whether it values having a paramedic service enough to pay for it, and if so, how it wants to achieve that change. One resident who works in another town’s fire department suggested to me several years ago that the town could give its current EMT’s three years to become paramedics. Becoming a paramedic requires a 1,400 hour training process: 600 hours of classroom work, 400 hours of clinical, and 400 hours of field work. Such a work change would have to go through the collective bargaining process. Alternately, the writer below suggest hiring eight new paramedics and having them run the town’s ambulance service, and having the current EMT’s remain as just firefighters. The MFD would thereby double its size.
Paul Enos <paul.c.enos@gmail.com>
To: eclarke@medfield.net
Dear Medfield Selectmen,
Evelyn Clarke <eclarke@medfield.net>
Mon, Oct 31, 2016 at 12:52 PM
I am writing to formally request the hiring of 8 firefighter/paramedics and the implementation of an Advanced Life Support ambulance be implemented to the Medfield Fire Department services. Many residents I have spoken with would like this matter added to the November 1st Town Meeting Agenda. It is a dangerous gap in our towns services and absolutely must be rectified immediately.
I would like to provide you a personal example of how ALS can impact the survival of a 911 patient. Seven years ago my father and I were working to replace some windows of his Needham home. After about an hour of work in the sun, my father collapsed. He immediately woke and told me he felt dizzy. I called 911 and moved him into a shaded area where I took his blood pressure, which fell to 50/null. How helpless I felt in the moments leading to that point – being a paramedic myself and having no equipment or manpower to help me find out what had gone wrong with my father. Every second felt like eternity, as it does when you are in a crisis. My father soon again went unresponsive when Needham Fire Department Paramedics arrived and began treatment. Within two minutes of patient contact, my father was properly assessed, placed on ECG monitoring, had an IV line established, and fluids initiated to bring his pressure up. It was discovered that his body reacted poorly to being placed on HCTZ (a diuretic) and when coupled with a hot day in the sun, lead to dangerously low blood pressure due to dehydration. If Needham paramedics had not responded and treated my father on site, I believe he would have died that day as his pressure was so low he was subject to cardiac arrest. My father, again, just this past year, required the Needham ALS ambulance when he fell and broke his forearm in 2 places, dislocated his elbow, and fractured his spine. The paramedics could not have moved him without administering narcotics to manage the immense pain he was in that day. ***Every stated skill that was performed on my father in these two instances, are ALS skills, and would not have been provided in the town of Medfield.*** Knowing my family has required these services in the past, and likely will again in the future, I would never recommend my parents move to Medfield. Not until the town adds ALS service to its fire department.
Having the experience of having worked as a paramedic for and along side private services over the past 8 years has given me a definitive perspective that every municipality is better seNed having public sector EMS service. Pr ivate services, as this town has learned recently, has one true interest – Profit. We are without ALS coverage, once again, because these services find our towns service area not to be profitable. They will emphasize how important patient care is to them and tell you what you need to hear to get the contract, but if you get inside those walls and experience how these services operate on a day to day basis, you and much of the public would be horrified to find how these services jeopardize the health and well being of the communities they service in order to turn a profit.
One glaring example I can provide is an incident where I took a transfer patient with my partner to a hospital more than 30 miles outside of our service area. While a competing ambulance service had more localized operating ambulances in several neighboring communities to that service area, my partner and I were still dispatched to an ALS response back in the town as we finished our transfer. We stated back to dispatch our distance from address, but we were told to continue in to the call. There were likely dozens of ambulances closer to that patient than we were, but they were not dispatched since they were working for a different company. This is how private ems functions. Services will not give up calls to competing ambulance services even if those units are significantly closer to the patient, as this forfeits the profits of that call to the competitor.
Additionally, Private EMS services are a continuous revolving door of personnel. In the world of private ems, staff are constantly switching companies, service areas, and career fields, leaving little if any continuity over the years. This is for many reasons – poor work conditions, poor pay, lack of quality leadership, and lack of benefits. This leads to massive problems with familiarity with a community, which in truth is half the battle working in a 911 service. Knowing where you are going. Knowing your surroundings and structures. Knowing which hospitals have which capabilities, and which would be the best point of entry for which patients. These logistical skills take great time and effort to ascertain and maintain and go well beyond using a GPS system. Having the same personnel working within your community and system for the length of their career offers enormous benefits relating to response times, community outreach, and continuity of care to town residents who frequently require these services due to chronic health problems. And who are those folks with chronic health problems? Children with special health concerns such as diabetes, asthma, allergies, and other ongoing medical conditions. Residents with disabilities, history of heart disease, and stroke. People who have had to experience medical emergencies first hand are fully aware of this gap in our towns capabilities.
When hired via civil service, employees typically remain with their departments for 30+ years, servicing the same community, working the same streets, and staying current with the changes in the community. They stay committed to their craft as they are provided a stable paying job with strong town benefits, and are integrated into the strong leadership a para-military structure provides in the fire department. They form strong relationships with their community and add the strength of continuity those private sector services lack. Most importantly, their number one priority is the health and well being of their patients. Profit is no longer a factor in clinical and logistical decision making.
Some residents may wonder, “Don’t we already have an ambulance on our fire department?” We do, but we do not have paramedics. A paramedic is a 911 responder who has undergone extensive training on the application of emergency medicine. ALS stands for Advanced Life Support, which is what a paramedic provides to it’s patients. Paramedics carry life saving medications and medical interventions that dramatically impact the survival of the patients they respond to. These services for Medfield have been covered via a regional contract provided by private ambulance services, which have now abandoned our town for the second time this year as we have been deemed by them to be a poor investment. This leaves us without coverage and relying on borrowing extended response times for ALS service from Walpole and Westwood.
Currently, Medfield has a BLS ambulance. BLS stands for Basic Life Support. It is operated by basic level Emergency Medical Technicians. While these staff members are also vital to a medical response, they do not carry the majority of the life saving medications and interventions that an ALS unit carries. The level of training for a BLS staff member is significantly less than is for ALS. BLS ambulances are essentially transport units that provide minimal measures in medical intervention. I will outline a two examples of vital differences is how BLS staff treat common medical emergencies versus how ALS treats them.
WHAT IS THE DIFFERENCE IN TREATMENT OF A HEART ATTACK?
If your town offers BLS, the BLS ambulance can provide Aspirin and Oxygen. They will always then call for an ALS Unit and hope one is available to meet them.
If your town offers ALS, they would administer the Aspirin and Oxygen. ALS would them provide a 12-lead ECG. This assists with pinpointing where in the heart the damage is taking place. Based of where the problem is in the heart, Paramedics typically administer Nitroglycerine. This medication opens the coronary arteries to help circumvent blood flow around a blockage in the heart, protecting the heart from cell death and minimizing the damage from a heart attack. ALS also provides IV access to administer narcotics for pain relief as chest discomfort from a heart attack can be significant, and alleviates the anxiety that further progresses damage to the heart. They can also provide blood pressure support with fluids through the IV if needed. These interventions are all time sensitive as with each passing minute, the heart incurs more damage ultimately resulting in disability and death. The sooner ALS reaches you, the more effective these treatments are and the greater chance you have for long term survivability.
WHAT IS THE DIFFERENCE IN TREATMENT OF CARDIAC ARREST?
If your town offer BLS, the BLS ambulance can provide CPR and an Automated Defibrillator. They will always then call for an ALS Unit and hope one is available to meet them.
If your town offers ALS, they would administer CPR and connect to an ECG monitor. With an ECG monitor, a Paramedic is trained to read what arrhythmia has caused the cardiac arrest, and administer the appropriate charge of electricity to treat that arrhythmia. Paramedics will also administer an IV to administer life saving medications that assist in restarting the heart into a normal rhythm. If an IV can not be started, which is the case in many sick patients with poor IV access, paramedics can also drill into the patients bone to administer these medications into the bone marrow. Paramedics will also intubate these patients for a controlled airway and monitor blood gas levels to ensure respiration are being provided as the patient needs them.
These differences in level of care continue through out all medical and traumatic protocols, and I would be happy to outline the difference in care in any medical or traumatic emergency you would like information on. Here is a reference link if you would like to read more treatment differences yourself.
http: //www.mass.gov/eohhs/provider/guidelines/resources/clinical-treatment/public-health-oems-treatment-protocols.html
It is easy to dismiss these differences in care until it is you or a loved one who is in need of these services. A medical emergency comes immediately and without warning, and is not an event a family can appropriately plan for. This is why you hire skilled responders – it is their job to be as prepared as possible for these emergencies. Every second matters when it comes to vital structures of the body. Having a responding public sector ALS services within our community is critical to our towns safety and well being. In addition to providing advanced life support to our community, these first responders would be cross trained as firefighters, as is typical of this addition, boosting our fire department to 4 members on shift instead of just 2.
Attempting to force our current firefighters to upgrade to ALS is unacceptable and not a viable option. Being a paramedic is a different job with different requirements. It is a decision that should be made by the individual. To be an effective paramedic, it is a training you must want fo obtain and maintain, and while our current fire department members are effective as Firefighter’s and EMT’s, being a paramedic does not translate for all in the field. Additionally, our two firefighters per shift are outnumbered in operating the three different typical responding apparatus – that is an engine company (which supplies water to a fire), a ladder company (which supplies an aerial ladder and ground ladders), and an EMS/Rescue unit. The NFPA (National Fire Protection Association) requires four personnel be staffed to each company for safe and effective operation. Therefore, our fire department should be advancing it’s staffing numbers, not bombarding it’s current members with more tasks when they are already undermanned. Hiring 8 Firefighter/Paramedics would bring our staffing per shift to 4 members, allowing them to at least safely operate any one responding company at one time. The distribution of that staffing and the logistics of how those apparatus respond is surely in great hands with our current fire department members under the leadership of Chief Kingsbury. Please see the NFPA staffing requirement outlined below:
“NFPA 1710 outlines the following minimum requirements for staffing fire suppression The activities involved in
controlling and extinguishing fires. services (based upon operations for a 2000 square-foot, two-story, single-family occupancy with no basement, exposures or unusual hazards):
“A minimum of four fire fighters per engine company. Fire companies whose primary functions are to pump and deliver water and perform basic fire fighting at fires, including search and rescue. or truck company. Fire companies whose primary functions are to perform the variety of services associated with truck work, such as forcible entry, ventilation, search and rescue, aerial operations for water delivery and rescue, utility control, illumination, overhaul, and salvage work. (§ 5.2.2.1.1).”
Though I have not conducted the research to confirm any financial figures, I read one statement by one selectman to be a $1.6 million startup cost. However the billing for the services of an ALS ambulance can help to offset some of the operation costs. Though those profits have proven not to be strong enough to hold a private service in place, the billing income would certainly be a strong contribution towards offsetting the expenses. We cannot go on having these gaps in service, and we cannot go on taking these services from our neighboring communities. I suggest to you that this is no longer a choice, but a necessity. Hiring another private service will only lead to another dropped contract, another gap in coverage, in addition to all the other stated problems that accompany a private service. It would continue leaving our valued fire department understaffed to perform their job. The citizens of Walpole and Westwood have been responsible enough to spend their tax dollars on an ALS ambulance, and every time we need them, we are robbing their community
of the services they pay to keep in place. We need to provide this service for ourselves, and to get our fire department to safe staffing levels. It is our responsibility to provide our emergency departments with the funding to operate their equipment at an emergency scene with safe levels of staffing. They are there to protect us, let’s do what we can to protect them.
It is time for us to act. The longer we wait, the more we invite a tragic outcome. It is time for us to upgrade our fire department and ems services to ALS by hiring 8 Full Time Firefighter/Paramedics to supplement the current hard working department.
Paul Enos
Firefighter/Paramedic
Cambridge Fire Department
Medfield Resident
paul. c. enos@gmail.com

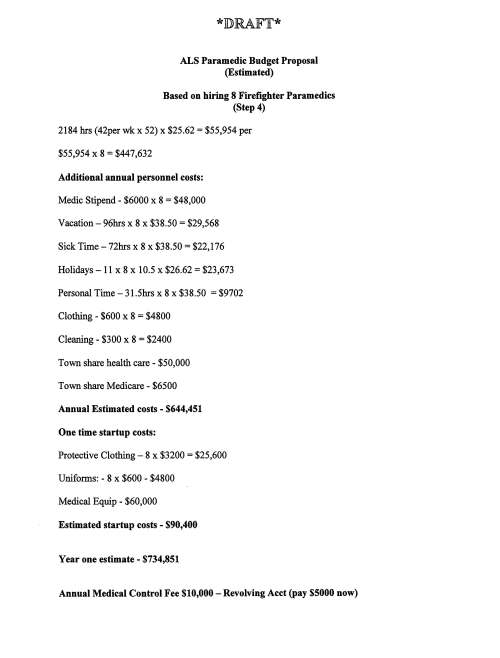

![*]])RAJF'Ir* ALS Paramedic Budget Proposal (Estimated) Based on hiring 8 Firefighter Paramedics (Step 4) 2184 hrs (42per wk x 52) x $25.62 = $55,954 per $55,954 x 8 = $44 7 ,632 Additional annual personnel costs: Medic Stipend - $6000 x 8 = $48,000 Vacation-96hrs x 8 x $38.50 = $29,568 Sick Time-72hrs x 8 x $38.50 = $22,176 Holidays-11x8 x 10.5 x $26.62 = $23,673 Personal Time - 31.5hrs x 8 x $38.50 = $9702 Clothing - $600 x 8 = $4800 Cleaning - $300 x 8 = $2400 Town share health care - $50,000 Town share Medicare - $6500 Annual Estimated costs - $644,451 One time startup costs: Protective Clothing- 8 x $3200 = $25,600 Uniforms: - 8 x $600 - $4800 Medical Equip - $60,000 Estimated startup costs - $90,400 Year one estimate - $734,851 Annual Medical Control Fee $10,000 - Revolving Acct (pay $5000 now)](https://medfield02052.blog/wp-content/uploads/2016/12/20161221-chief-kingsbury-als-paramedic-budget-proposal.jpg?w=500)